Erythroderma
- Home
- / Erythroderma
🔺Q1: What are the drugs causing erythroderma?
✅Ans: Anti convulsants – phenytoin , carbamazepine pheobarbital
ACE inhibitors- Captopril
Antibiotics – doxycycline, demeclocycline
Anti malarials – chloroquine, hydroxy chloroquine
NSAIDS
Arsenic
Gold
Beta blockers
Beta carotene
Dapsone
🔺Q2: What is the difference between acute and chronic erythroderma?
✅Ans: Acute erythroderma there is skin faliure resulting in lufe threatening systemic upset.
chronic erythroderma systemic complications are less frequent
🔺Q3: What are the complications of erythroderma?
✅Ans: Hypothermia
Electrolyte abnormalities
Dehydration
Red skin leads to high-output heart failure.
A secondary skin infection like impetigo & cellulitis
General unwellness can lead to pneumonia
Hypoalbuminaemia from protein loss and increased metabolic rate causes oedema
Longstanding erythroderma may result in pigmentary changes (brown and/or white skin patches)
🔺Q4: What is papuloerythroderma of Ofuji?
✅Ans: This distinctive pattern of erythroderma differs from ordinary erythroderma in that papulation is prominent, it tends to spare the face and flexures, and is often intensely pruritic.A characteristic and distinctive pattern of sparing of the abdominal flxures has been termed the ‘deck chair sign’.Additional features often observed include hyperkeratosis and fissuring of the palms and soles, and benign lymphadenopathy. There is usually circulating eosinophilia and a raised IgE, as well as a mild degree of absolute or relative lymphocytopenia. It mainly affects males and typically persists for years.
🔺Q5: What are the infections that can lead to development of erythroderma?
✅Ans: Dermatophyte infection such as Trichophyton violaceum
HIV infection
crusted scabies
🔺Q.6: What is Leiner’s disease (erythroderma desquativum/ red scaly syndrome)?
✅Ans:
- Failiure to thrive-
- Low birth weight-
- Diarrhoea-
- Erythroderma-lesions similar to seborrheic dermatitis
🔺Q7: What is the cause of Hairloss in erythroderma?
✅Ans:
🔸Hypoproteinemia due to loss of scales
🔸Hyperestrogenemia
🔸Loss of sulphur in scales
🔺Q8: What is Red Man Syndrome?
✅Ans: It is characterized by dermatopathic lymphadenopathy, palmoplantar keratoderma and relapsing erythroderma.
🔺Q9: Psoriatic Erythroderma Management
✅Ans: In psoriatic erythroderma low dose methotrexate , acitretin or ciclosporin can be given.avoid topical tar and uv therapy.
🔺Q10: What are the causes of erythroderma in neonate?
✅Ans:
🔸Infantile seborrheic dermatitis.
🔸Atopic dermatitis.
🔸Psoriasis.
🔸Pityriasis rubra pilaris.
🔸Ichthyosis: nonbullous ichthyosiform erythroderma, Conradi-Hünermann syndrome, bullous ichthyosiform erythroderma.
Netherton syndrome
🔺Q11: What are the nutritional requirements of an adult in erythroderma?
✅Ans: Daily requirement of protein is 2 to 3g/kg/day. if 70 kg man then 140g
Morning:
2eggs= 8gm
1cup milk= 8gm
1 leg piece= 24gm
1 cup pulse = 16gm
Lunch :
Above all except leg piece
Dinner :
Above diet
🔺Q12: How to calculate fluid requirements of an adult in erythroderma?
✅Ans:
0.7ml/kg /% of affected body surface area and 5%albumin
1ml/kg/ %of body surface area invloved titrated to maintain urine output .5 to 1ml/kg/h. It is monitored according to urine output 0.5 to 1ml/kg/24hr
🔺Q13: What will be the TNM stage and Clinical stage of a patient in erythroderma with MF?
✅Ans: Clinical stage = 3A and 3B
TNM = T4 N0-x M0-1
🔺Q14: What is the most common cause of erythroderma in psoriatic arthritis?
✅Ans: Abruptly stopping psoriasis treatments, like corticosteroids or immunosuppressants,
🔺Q15: What is dermatopathic lymphadenopathy?
✅Ans: Reactive lymphadenopathy characterized by paracortical expansion with increased interdigitating dendritic cells, Langerhans cells and histiocytes / macrophages, typically including melanophages.Typically associated with chronic skin irritation, inflammation or infection.
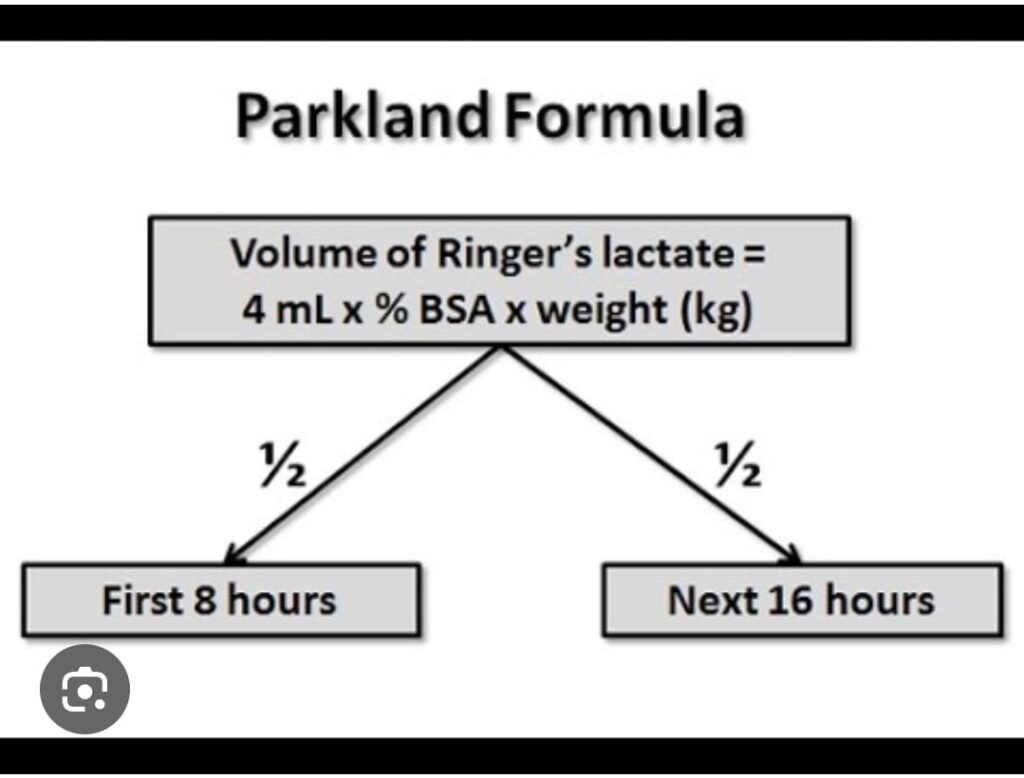
🔺Q16: What is parkland formula
✅Ans: see pic below
🔺Q17: What is concealed pyrexia in erythroderma?
✅Ans: Increased skin perfusion leads to thermoregulatory disturbances. Shivering and hypothermia may occur even though the skin feels deceptively warm, also known as concealed pyrexia.
🔺Q18: What is the Significance of eosinophillia in erythroderma?
✅Ans: Eosinophilia may be due to underlying lymphoma so its a prognostic marker for death in erythroderma
🔺Q19: What is pavithran sign?
✅Ans: Seen in erythroderma in which there is complete absence of erythema and scaling of the nose and perinasal areas.

🔺Q20: When is skin biopsy done in erythroderma?
✅Ans: skin biopsy is done to reveal the underlying cause after the acute erythroderma settles however some authorities recommend that even in erythroderma biopsy may give a clue to underlying malignancy like lymphomas .
🔺Q21: What is the Role of antibiotics in erythroderma?
✅Ans:
🔸Secondary infections:
Antibiotics should be used with caution as they can be a cause of erythroderma.if secondary skin infections evident then start antibiotics after taking C/S.
🔸Prophylactic use:in immunoconpromised patients or those with severe disease
🔺Q22: What are the Bad prognostic signs in eryhthroderma?
✅Ans:
🔸Persistent fever
🔸Age more than 60
🔸Comorbidities:
immunocompromised,
cancers, autoimmune disorders
🔸Pancytopenia
🔸drugs with prolong half life
🔸Resistant to treatment
🔺Q23: Cause of death in erythroderma?
✅Ans: Pneumonia
🔺Q24: What is the Difference in lymphadenopathy of erythroderma and MF?
✅Ans: In erythroderma there is dermopathic lymphadenopathy, benign histiocytic infiltration in paracortical area of lymph nodes while in MF there are atypical lymphocytes aggregates leading to effacement of nodes
🔺Q25: What are the Causes of rapid onset erythroderma?
✅Ans:
🔸Drugs
🔸infections
🔸psoriasis
🔸carcinoma:leukemia/lymphoma
🔺Q26: What are the bullous cause of erythroderma?
✅Ans:
Bullous Causes of Erythroderma
Erythroderma, or exfoliative dermatitis, can have several bullous (blistering) causes, including:
Bullous Causes of Erythroderma
Pemphigus vulgaris
An autoimmune blistering disorder affecting the skin and mucous membranes.
Bullous pemphigoid
Another autoimmune blistering disorder, more common in the elderly.
Stevens-Johnson syndrome (SJS)/Toxic epidermal necrolysis (TEN)
Severe mucocutaneous reactions, often triggered by medications or infections.
Drug reactions
Certain medications can cause bullous drug eruptions leading to erythroderma.
Staphylococcal scalded skin syndrome (SSSS)
A bacterial infection that can cause widespread blistering and erythroderma, primarily in infants and young children.
🔺Q27: What is the Role of Antibiotics in Erythroderma and Indications?
✅Ans: Antibiotics can be used in the management of erythroderma under specific conditions:
Secondary Infection
If there is a secondary bacterial infection, systemic antibiotics are indicated.
Primary Infective Causes
In cases where erythroderma is due to an underlying infection like SSSS, appropriate antibiotics targeting the causative organism (e.g., Staphylococcus aureus) are necessary.
Prophylactic Use
Sometimes, prophylactic antibiotics may be considered to prevent secondary infection in severe cases, though this is less common.
🔺Q28: Which Interleukins are Involved in the Pathogenesis of Erythroderma?
✅Ans:
IL-1:
Promotes inflammatory responses, fever, and acute phase reactions.
IL-2:
Essential for T-cell proliferation and differentiation, which can contribute to the inflammatory milieu in erythroderma.
🔺Q29: What is Management of a Patient with Erythroderma?
✅Ans: Step-by-Step Approach
Assessment and Diagnosis
History:
Detailed drug history.
History of pre-existing dermatologic conditions.
Recent infections or systemic symptoms.
Physical Examination:
Extent and distribution of erythema.
Presence of blisters, scales, and erosions.
Lymphadenopathy, hepatosplenomegaly.
Laboratory Tests:
Complete blood count (CBC) to check for infection, anemia.
Liver and renal function tests.
Electrolytes to monitor for imbalances.
Skin biopsy for histopathological examination.
Stabilization
Fluid and Electrolyte Management:
IV fluids to correct dehydration.
Monitor and correct electrolyte imbalances.
Temperature Regulation:
Maintain a warm environment to prevent hypothermia.
Identification and Management of Underlying Cause
Withdraw Potential Offending Agents:
Immediate cessation of suspect medications.
Specific Treatments:
Psoriasis:
Systemic treatments like methotrexate, cyclosporine, or biologics.
Atopic dermatitis:
Systemic corticosteroids, immunosuppressants.
Infections: Appropriate antibiotic or antiviral therapy.
Symptomatic Treatment
Topical Treatments:
Emollients to restore skin barrier.
Topical corticosteroids to reduce inflammation.
Systemic Treatments:
Systemic corticosteroids (e.g., prednisone) for severe inflammation.
Immunosuppressants or biologics depending on the underlying condition.
Monitoring and Supportive Care
Regular Monitoring:
Vital signs, fluid balance, skin condition.
Nutritional Support:
Ensure adequate calorie and protein intake.
Infection Prevention:
Strict skin hygiene, use of antiseptic solutions.
Consider systemic antibiotics if secondary infection is suspected.
🔺Q30: Can PUVA Therapy be given to patient in Erythroderma?
✅Ans:
Indications:
PUVA may be considered in stable patients with psoriasis, CTCL, or other phototherapy-responsive conditions.
Risks:
High risk of infection, delayed wound healing, and potential exacerbation of symptoms if used in the acute phase.
Caution:
Should be introduced cautiously and under strict medical supervision, typically once the patient is stabilized.
Secondary candidate 1
1🔺Cause of protein loss in erythroderma
▪️Increase catabolism
▪️Decrease synthesis
▪️Shedding of scales
▪️Dilution
▪️Enteropathy
2🔺how to calculate fluid requirement of an adult in erythroderma
▪️Initial 24 hours: N/S 0.7 ml/kg per BSA
Thereafter gradually decrease fluids
3🔺what is leiners disease/ red scaly syndrome
▪️Leiner disease occurs in infants and is characterised by severe generalised seborrhoeic dermatitis, recurrent diarrhoea, recurrent skin and internal infections, and failure to thrive. It is also known as erythroderma desquamativum. Leiner disease may be present at birth but more commonly develops within the first few months of life. It appears to be more common in females than males.It is caused by a defect in the body’s complement system.
4🔺effect of nails due to drug induced erythroderma
▪️there are bands of nail plate discontinuity
Shoreline nails
Leukonychia
5🔺why there is hair loss in erythroderma
▪️telogen effluvium
▪️hypoproteniemia
▪️sulphur deficiency
Q1.How to differentiate between lymphadenopathy of papulo erythroderma of ofuji and sezary syndrome ?.
ANSWER:In papuloerythroderma of ofuji superficial lymph nodes appears few months later and peripheral T cell non epidermotropic skin lymphoma occurs and in case of MF in lymph nodes biopsy complete effacement of nodal architecture by sezary cells.
Question 2.what are causes of erythroderma in neonates ?
ANSWER:causes include:
Infected seborrheic dermatitis
Pityriasis rubra Pilaris
Psoriasis
Generalized mastocytosis
Non bullous icthysiform erythroderma
Netherton syndrome
Toxic epidermal necrolysis
Staphylococcal scalded skin syndrome
Omenn syndrome
Question 3.Indication of steroids in erythroderma?
Answer:Steroids are only given in case of severe disease.
Question 4 :Can puva can be given to patient in erythroderma?
Answer:Yes puva can be given in patients of erythroderma
Question 5.Bad prognostic sign in erythroderma?
Answer:The disease course is rapid if it results from drug induced;lymphoma ,leukemia,contact allergies and staphylococcal scalded skin syndrome .in acute eythroderma skin failure is life threatening Fever is poor prognostic marker and may lead to severe deterioration .
Question 6.Cause of edema in erythroderma?
ANSWER:Hypoalbunemia from protein loss and increase metabolic rate causes edema.
Secondary candidate 3
. drugs causes erythroderma
Sulphanomides,nsaids, allopurinol,att, anticonvulsant, vancomycin, Cephalosporins
- Ideally we have to do biopsy once erythroderma is settled.we can do multiple serial biopsies during erythroderma to rule out the cause but only it identify the cause in 50%
In acute stages there is spongiosis and para keratosis and in chronic cases there is elongation of rete ridges. - Daily protein requirement in erythroderma. 1.5-2gm/kg/day
- Mechanism of high output cardiac failure. high-output cardiac failure develops due to a combination of increased systemic blood flow and a decreased systemic vascular resistance. The skin’s increased blood flow in erythroderma leads to shunting of blood into the peripheral circulation, bypassing the normal capillary network, thus reducing systemic resistance. This, coupled with potential metabolic demands from systemic inflammation, can overwhelm the heart’s desire and it will lead to high output cardiac failure
- Causes of glucosuria in erythroderma
Pancreatitis causing decreased insulin secretion
Peripheral insulin resistance
Stress
Infections
Secondary candidate no 3
🛑 What are the infectious causes of erythroderma?
🟢
- Norwegian scabies
- Dermatophytosis
- Staph scalded skin syndrome
- Viral exanthems
- Candidiasis
- HIV
🛑 what’s are complications and causes of complications of erythroderma?
🟢 Main complications of erythroderma are following
- High output cardiac failure due to increased skin perfusion.
- Hypothermia
- Hypoalbuminemia due to increased protein loss from scales.
- Peripheral edema due to hypoalbuminemia and capillary leakage.
- Dehydration, Electrolyte imbalance due to increased fluid loss and perspiration.
- Cutaneous, subcutaneous infections
- Respiratory infections, pneumonia being the commonest cause of death.
🛑what is pavithran sign?
🟢 It is sparing of nose and paranasal areas in erythroderma.
🛑 what is concealed pyrexia?
🟢 In erythroderma skin already feels warm because of increased peripheral skin perfusion, so even if patient gets fever, it’s not noticed , this is concealed pyrexia. Therefore the rectal temperature must be taken.
🛑what is redman syndrome?
🟢 Red Man Syndrome is characterized by dermatopathic lymphadenopathy, palmoplanter keratoderma and relapsing erythroderma.
Sources: Rooks 10th edition and DYP survival guide.
💠 secondary candidate #5
1:What is leiner disease?
Leiner disease in which SD is typically severe and widespread and occurs in association with recurrent infections, failure to thrive and defi ciencies of various complement components.
💠 What is Alibert-Bazin disease?
Alibert-Bazin disease is an older name for Mycosis Fungoides, the most common type of cutaneous T-cell lymphoma (CTCL).
💠 What is shoreline nails?
Shoreline nail refers to a pattern where the nail plate shows transverse pigmentation or ridging, resembling the irregular edge of a shoreline. It is typically seen as a result of temporary interruption of nail matrix activity, often due to systemic stress like chemotherapy.
💠 What is ebonization?
a darkening or blackening of the nails, often described as a shiny, blackish appearance. This phenomenon is most commonly observed in cases of erythroderma.
💠 Causes of Erythroderma in children?
Atopic dermatitis
Psoriasis
Omen syndrome
Netherton syndrome
Icthyosiform erythroderma